[Type text] [Type text] [Type text]
2
HEALTH ASSESSMENT
The process of evaluating the health status by inquiring the health history and performing the physical exam is known as health assessment. Pseudo name is used to uphold the confidentiality of the client. In accordance with College Of Nurses Of Ontario (2009) nurses have moral and lawful obligations to look after the secrecy and protecting the client health data acquired while providing care. This paper discusses the results of the demographic and historical, subjective and objective data acquired while performing the assessment.
Mrs. K is 89 years old with history of stroke, atherosclerotic heart disease, congenital urinary deformity (CUD) and hypertension (HTN). She is also diagnosed with diabetes, asthma and arthritis. Mrs. K resides at York Extendicare. Her glucose levels are monitored everyday. Due to her medical history resident sometimes experience shortness of breath (SOB), anxiety and restlessness. Mrs. K has a mobility limitation as she is one-person transfer and is in wheelchair.
 grasp reflex of a 5 month old baby boy.
grasp reflex of a 5 month old baby boy.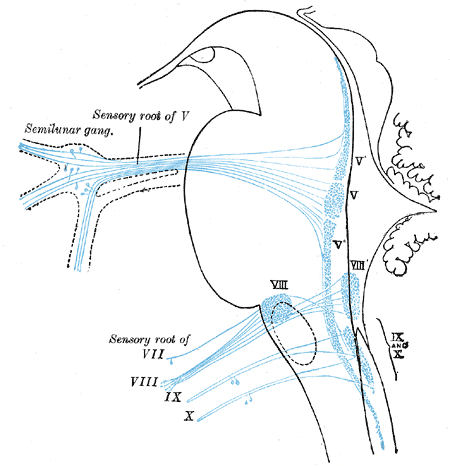 Primary terminal nuclei of the afferent (sensory) ...
Primary terminal nuclei of the afferent (sensory) ... Nuclei of origin of cranial motor nerves schematic...
Nuclei of origin of cranial motor nerves schematic...Mrs. K is also at a risk of falls. She requires extensive assistance by a health care aid to complete all aspects of hygiene. Mrs. K can wash her face and hands with some cueing and guidance. She is on diabetic regular diet. She wears prescribed glasses. She also wears dentures. Neurological assessment was performed on Mrs. K. The purpose of a neurological assessment is to detect neurological injury in the patient, monitor its progression to determine the type of care to provide, and gauge the patient's response to the interventions (Noah, 2004). Neurological assessment was done on Mrs. K since she presented left side hemiplegia following the stroke 34 years ago. Stroke results in acute loss of neurological function due to an abnormal perfusion of brain tissue (Jarvis, 2009, p. 696). The initial evaluation covered several critical...