There are a few different procedures for kidney stones. The procedures depend on there size and location.
About 80% of ureteral stones pass spontaneously in the urine, usually within 48 hours of the acute attack. Most patients can be managed as outpatients. Conservative treatment consists of reassurance, adequate pain control, and advice to maintain adequate hydration. A three-day supply of an oral narcotic analgesic such as hydromorphone can be prescribed and the patient told to return immediately if severe, intractable pain, persistent nausea and vomiting, or fever and chills occur. A urine strainer should be prescribed and patients instructed to strain all urine for up to 72 hours after the pain subsides to try to retrieve the stone for analysis. If a patient is unable to pass the stone they may need to have them removed with Laser lithotripsy, Percutaneous nephrolithotomy or Ureteroscopy.
Laser lithotripsy (a non-invasive removal technique) has become the method of choice and most widely used approach for removal of Kidney stones.
 Patient Recognition Month Poster
Patient Recognition Month Poster Bilateral kidney stones on abdominal X-ray. Not to...
Bilateral kidney stones on abdominal X-ray. Not to...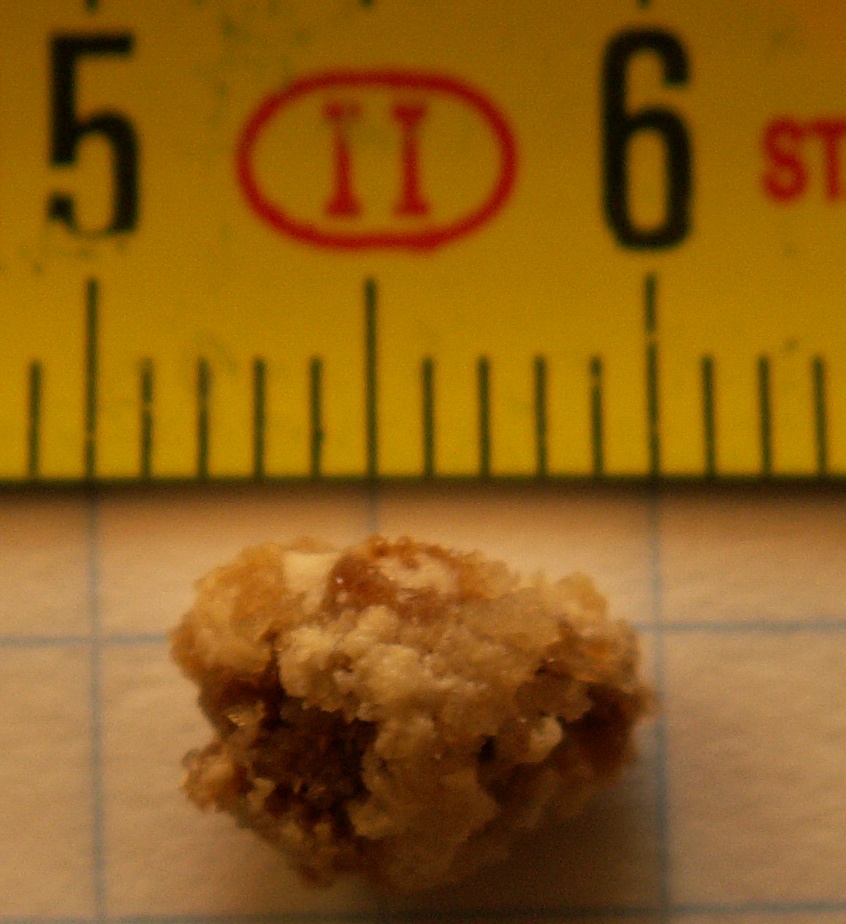 Kidney stone
Kidney stoneThe technique is appropriate for almost all calculi in the renal collecting system and some of those in the upper ureter. Renal calculi of 2 cm or less are the ideal targets. Lithotripsy makes use of shock waves generated by an underwater spark discharge and focused by a hemielliptic reflector. The patient is manipulated into position within a water bath so that the targeted stone visualized on a fluoroscopic monitor is at the focal point of the concentrated shock waves. About 1,000-2,000 shocks are needed to fragment a stone into sand like particles, which can then be passed in the urine. The procedure usually lasts about 60-90 minutes and requires general, epidural, or spinal anesthesia. Most patients can be discharged the same evening and return to work after a few days.
Percutaneous nephrolithotomy is used principally in patients with renal or upper ureteral stones that are not suitable for lithotripsy. This procedure is used when the size of the stone is larger than 2 cm, hardness (cystine stones), or complexity (infection stones). Percutaneous nephrolithotomy requires general anesthesia. Under fluoroscopic or ultrasonographic guidance, an 18-gauge needle is introduced into the renal pelvis through the flank, then replaced with a fine guide wire that permits the placement of a dilating catheter to establish a nephrostomy tract. A rigid or flexible nephroscope can then be introduced through the tract to visualize the stone. Stones less than 1 cm in diameter can be grasped directly using a basket or forceps and extracted through the operating channel of the nephroscope, although stones this size are usually treated with lithotripsy. With larger stones, an ultrasonic or electrohydraulic lithotripsy probe is introduced through a channel of the nephroscope and placed in direct contact with the stone to reduce it to fragments. After removal of the nephroscope, the nephrostomy tract is usually maintained with a nephrostomy catheter until a nephrostogram can be obtained two or three days later. If no obstruction or extravasations appears, the tube is clamped and removed the next day and the patient can be discharged.
Ureteroscopy is the method of choice for removing stones lodged in the lower third of the ureter. In this procedure, a rigid or flexible ureteroscope is advanced over a guide wire (sometimes after ureteral dilation using a balloon dilating catheter) up through the urethra, ureterovesical junction, and ureter to the level of the stone. Small stones can be extracted by a basket or forceps introduced through the ureteroscope. Stones too large to pass are first fragmented by an ultrasonic lithotripsy probe inserted through the ureteroscope, with continuous irrigation and suction through the probe to prevent thermal injury and aspirate stone fragments. Most ureteroscopic procedures can be done on an outpatient basis or require at most 24-48 hours of hospitalization.
Work SitedLingeman, James E., Glenn M. Preminger, and David M. Wilson. "Kidney stones: acute management." Patient Care 24.n13 (1990): 20-37. General OneFile. Gale. Spartanburg Community College RPA. 21 June 2009.
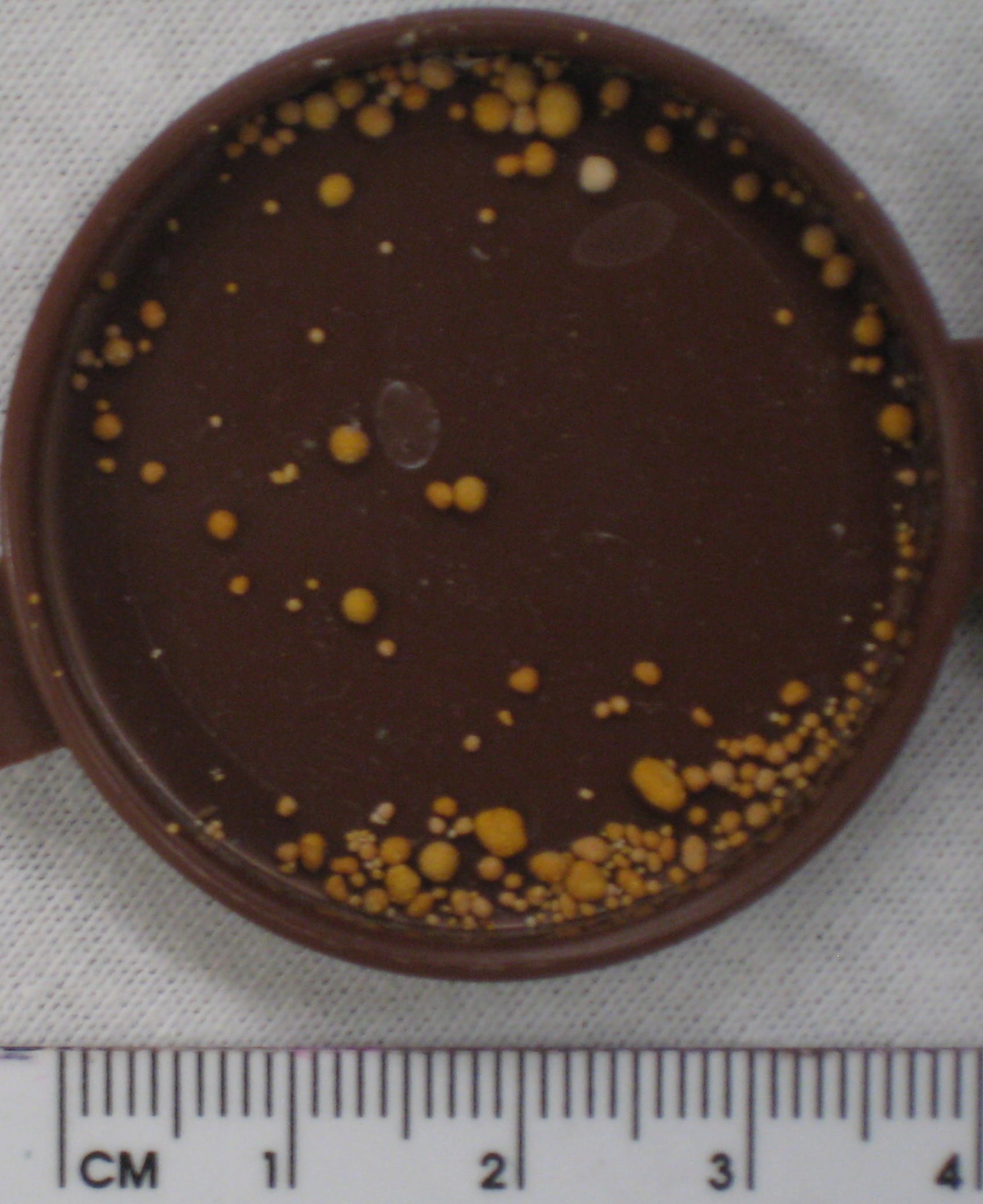 English: Muitiple kidney stones composed of uric a...
English: Muitiple kidney stones composed of uric a...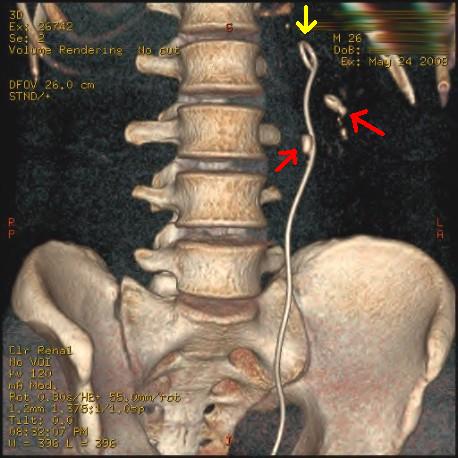 Three-dimensional reconstructed CT scan image of a...
Three-dimensional reconstructed CT scan image of a... English: KUB Radiograph showing a large staghorn c...
English: KUB Radiograph showing a large staghorn c...