Published: 1 Peninsula NIHR Clinical Research Facility, Peninsula Medical School, Exeter, UK, and Clinical Chemistry, Royal Devon and Exeter NHS Foundation Trust, Exeter, UK2 Peninsula NIHR Clinical Research Facility, Peninsula Medical School, Exeter, UK3 Clinical Chemistry, Royal Devon and Exeter NHS Foundation Trust, Exeter, UKTitle: Stability and Reproducibility of a Single- Sample Urinary C-Peptide/Creatine Ratio and its Correlation with 24-h Urinary C-peptide.
IntroductionThe research is a clinical and correlation experiment to determine how stable C-peptide is in urine. For every One C-peptide produced, there is an equal amount of insulin molecule produced in the pancreatic beta cell when pro insulin splits into insulin. Therefore knowing the amount of urinary C-peptide (UCP) present in a 24hrs urine sample tells us about the production rate of insulin in the individual. C-peptide is measured rather than insulin because it has a longer half life.
Materials and Methods:The research group analyzed UCP using a routine electrochemiluminescence immunoassay in samples obtained from 21 healthy volunteer, the stability of UCP with preservatives (boric acid, sodium azide and sodium carbonate) were compared as well as the reproducibility of urinary C-peptide/creatinine ratio (UCPCR) in first- and second-void fasting urines within a 24-h collections.
 Exeter CRE 006
Exeter CRE 006 Exeter CRE 001
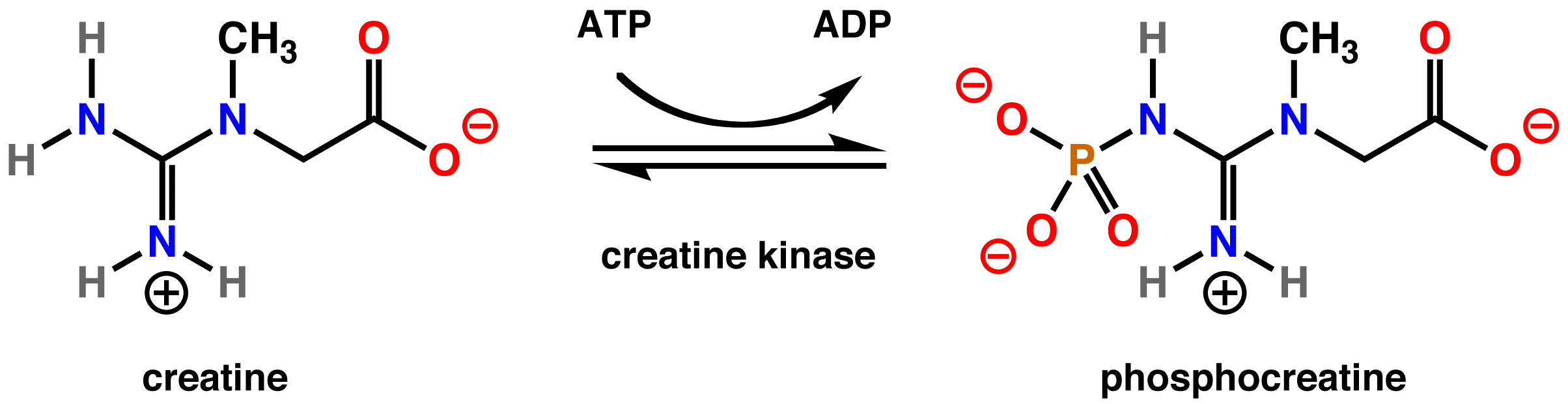
Exeter CRE 001 Creatine Kinase (Rabbit) Converts the major storag...
Creatine Kinase (Rabbit) Converts the major storag...My comment:The researchers could have analyzed C-peptide using some other techniques to ensure and compare the highest specificity and sensitivity of C-peptide not just limiting their technique using routine electrochemiluminescence immunoassay, methods such as:1. Two dimensional reverse phase/reverse phase high-performance liquid chromatography.
2.N- Terminal sequence analysis of endoproteinase Lys_C peptide map usine routine 3.5 method on the HP G1005A N- terminal protein sequencing system.
3.Other methods include: the Adaltis, RIa, the Dako Elisa, the PerkinElmer times-resolved fluoroimmunoassay and in house immunochemiluminometric assay4.The researchers did not mention if it was the free or bound C-peptide that was measured. Ethanol is efficient to differentiate and separate bound and free C-peptideResults:UCPCR stable at Room temperature for 24hrs at 4 degree centigrade for 72hrs2nd void fasting sample median = 0.78Second-void fasting UCPCRs were lower than first-void (median 0.78 vs 1.31, P = 0.0003) and showed less variation (CV 33% vs 52%), as second-void UCPCRs were not influenced by evening food-related insulin secretion.
Second-void fasting UCPCR was highly correlated with 24-h UCP (r = 0.8, P = 0.00006).
Study participantMy comment:1.The research team could have used a wider range of people, because the larger the size the better the results can be analyzed. 30 is the rule of thumb when considering sample size. A wider age range could have been used as well, not just limiting the age between 24-54yrs. for example monitoring the C-peptide in fetus or infants can show if there are differences and progression due to growth or whether there is an acquired or genetic problem.
2.The parameters for healthy patient were not well defined for example if patients are disease free, transplant patients, or if their organs such as the kidneys are working properly. The races of the healthy patients were not mentioned, because there might be genetic variation in regards to insulin metabolism. Diet could also play a role in insulin production, the type of food the participant eat were not mentioned or monitored. For example, patients who predominantly eat food high in carbohydrate, their blood sugar tend to rise to excessive levels, which create a condition known as insulin resistance, subsequently affecting the rate of insulin production. High levels of C-peptide also are seen with insulinomas (insulin-producing tumors) and may be seen with hypokalemia, pregnancy, Cusings syndrome and renal failure.
3.The research team only looked at the C-peptide in healthy patients. They could have compared data with those of unhealthy patients to see the differences in C-peptide production. Patients who are type 1 diabetic experience an autoimmune process that often starts in early childhood and involves the almost complete destruction of the beta cells ( involved in the production of insulin) over time. Eventually, little or no insulin (and C-peptide) is produced. In type 2 diabetics, the patients are insulin resistant so there is a compensatory increase in insulin production and release that can also lead to beta cell damage. Therefore the production rate of C-peptide will vary in these two different groups of diabetic patients.
4.How the patients fasted was not well defined by the research group, the time limit of fasting can affect the production of C-peptide. Also stress is another factor that can affect C-peptide production and it wasnÃÂt mentioned in the paper.
Creatine RatioMy comment:Different types of creatine occur in the body such as creatine monohydrate and creatine kinase (CK) also known as creatine phosphokinase (CPK). Elevation of CK is an indication of damage to many other diseases not only limited to problems with C-peptide. For example lowered CK can be an indication of alcoholic liver diseases which can cause fatty change, or macrovesicular steatosis. The research group did not mention the specific type of creatine they measuredIn conclusion, I donÃÂt think the research was adequately conducted. If the research group increased the range of people they used for the study and employed other techniques to compare specificity and sensitivity of C-peptide, as well as including unhealthy patients (type 1 and 2 diabetics) in their study, the values of the reproducibility and stability of C-peptide will subsequently be affected.
Work citedhttp://www.clinchem.org/cgi/content/abstract/55/11/2035http://www.chem.agilent.com/Library/applications/59653465.pdfhttp://www3.interscience.wiley.com/journal/112468890/abstracthttp://www.clinchem.org/cgi/reprint/54/6/1023.pdf
 Українська: Схема 1 — Метаб�...
Українська: Схема 1 — Метаб�... English: Hospital building, Heavitree Road, Exeter...
English: Hospital building, Heavitree Road, Exeter... A porcine islet of Langerhans. The left image is a...
A porcine islet of Langerhans. The left image is a...