History, Impact and EpidemiologyIn 1908, untold numbers of slaves and laborers working the railroads connecting Rio, Brazil to the heart of the Amazon succumbed to malaria, yellow fever and other mysterious, undiagnosed illnesses. Having been previously successful at reducing malarial disease transmission in the Santos shipping industry four years earlier, Carlos Chagas was appointed the challenge of alleviating the infectious disease burden being faced in the Brazilian interior. Upon relocating to the undeveloped, rural area of Lassance, he encountered droves of individuals complaining about irregular heartbeats, atypical arrythmias, cardiac insufficiencies and inexplicable cases of sudden death. Chagas had received training in fields of public health and parasitology from renowned physician, Oswaldo Cruz, and wisely deduced a link between the endemicity of myocardial failure and the triatomine bug. While unheard of along the more developed Brazilian coast, these large black insects would often emerge from cracked mud walls and thatch roofs to feed on the blood of inhabitants throughout the night.
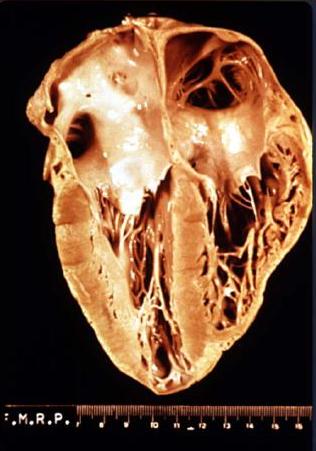 Gross anatomy of a heart that has been damaged by ...
Gross anatomy of a heart that has been damaged by ...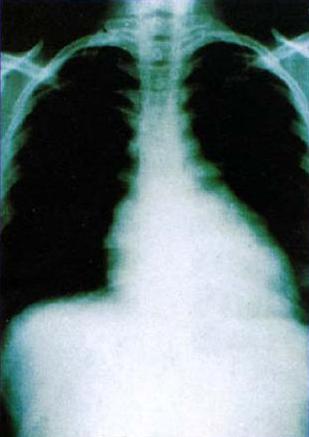 Chagas heart, radiology
Chagas heart, radiology Chagas in Latin America (A:Endemic zones)
Chagas in Latin America (A:Endemic zones)They were often referred to as ÃÂkissing bugsÃÂ for the trademark swollen bite sites often left near the eyelids and lips of their victims. Upon dissection of the triatomine bug, Chagas discovered a eukaryotic, flagellated protozoan similar to Trypanosoma brucei, earlier identified as the agent of African sleeping sickness. After finding this parasite in the bloodstream of young girl who had experienced fever, lymphadenopathy, hepatosplenomegaly and heart failure prior to death, after being been bitten by the reduvvid bug, Chagas confirmed the link between his novel trypanosome discovery and disease by infecting monkeys with triatomine droppings and observing identical clinical symptoms(Prata, 1994) Chagas named the protozoan after his mentor, Trypanosoma cruzi, and the associated disease eventually bore his own name. After nearly a century of its identification, Chagas disease remains a significant public health issue and a major cause of suffering and death in Latin America. The Centers for Disease Control estimates that 8 ÃÂ 11 million people in Mexico, Central and South America have Chagas disease and many are unaware they are even infected (http://www.cdc.gov/chagas/factsheet.html). The large numbers of currently infected individuals, along with the estimated 100 million at risk in 21 countries and approximate 50,000 annual fatalities, make T. cruzi infection one of the leading causes of heart disease and cardiovascular-related deaths in endemic areas (1-3). Public health efforts geared toward limiting vectorborne transmission have significantly reduced the number of newly infected individuals, but the cases now being identified outside of the typical endemic regions from increasing incidences of blood transmission (4) and organ transplantation (5) still make Chagas one of the most important diseases to understand due to its history of morbidity and mortality (6). Despite its obvious clinical importance and the efforts of many investigators, the pathogenesis of Chagas heart disease is still elusive due to the complex nature of the hostparasite interrelationship and numerous pathogenic mechanisms that have been proposed over the last century of research(Moncayo, 1999).
Trypanosoma cruzi ÃÂ Life cycle and TransmissionThe life cycle of T. cruzi involves two intermediate hosts (triatomine insects and mammals) and three well-defined morphological and functional developmental stages: epimastigotes, trypomastigotes and amastigotes. As illustrated in Figure 1, the epimastigote forms replicate in the midgut of the reduviid bug insect vector and develop into nonreplicative metacyclic trypomastigote forms residing in the vector hindgut. When the insects feed on blood, they release their excreta containing metacyclic trypomastigotes that subsequently penetrate the mammalian host through either scratching of the bite wound or permissive mucosa or conjunctival membranes and initiate cellular invasion. Trypomastigotes survive the acidic parasitophorous vacuole and freely enter the host-cell cytoplasm where they differentiate into the replicative amastigote form. Following many rounds of multiplication by binary fission, the cell cytosol fills with amastigotes which ultimately transform into bloodform trypomastigotes. A fully parasitized cell will then rupture, releasing trypomastigotes to the blood stream where they can either infect adjacent cells, disseminate through the blood, or be taken up by a new reduviid bug, thus completing the cycle. A less common, yet increasingly significant, route of parasite transmission is through transfusion of blood products(Revelli, 1999). As such, Chagas disease has become a potential problem associated with migration of infected individuals from endemic areas to the United States, Canada, Eastern Europe, Australia and Japan. Fortunately, the appropriate selection of blood donors, the use of more sensitive and accurate advanced molecular diagnostic tests and the application of a mandatory quality assurance system have improved the safety of blood banks in Latin American and have reduced the overall risk of acquisition of blood-borne Chagas disease.
Acute and chronic Chagas diseaseThere are typically two stages of infection in human Chagas heart disease: the acute stage which occurs shortly after the infection and the chronic stage which appears after a silent period that may last many years. The acute stage of the disease, generally seen in children, is characterized by fever, lymphadenopathy and hepatosplenomegaly, muscle and joint pains, malaise, respiratory disturbances and local inflammation at the site of infection. Focal cardiac inflammation and heart enlargement, attributed to mononuclear cell, mast cell and neutrophil infiltration, has also been observed (16). In nearly 95% of cases, clinical symptoms are either absent or mild and non-specific (6), making it difficult to diagnose disease in the acute stage of infection. In instances when symptoms manifest, less than 5% of individuals can succumb to infection, typically of either myocarditis or meningoencephalitis. More commonly, acute cases with or without symptoms progress to a chronic stage, where T. cruzi establishes a lifelong, low-grade infection which can present in any age group (6). Interestingly, two thirds of individuals harboring chronic parasite infection, often termed ÃÂindeterminateÃÂ, fail to demonstrate any detectable clinical signs and do not die of Chagas disease. However, in about one-third of cases(Prata, 1994), a chronic form of disease develops, causing irreversible damage to the heart, esophagus and colon, with dilatation and disorders of nerve conduction of these organs. The infiltrate in chronic Chagas heart disease primarily consists of lymphocytes with lower numbers of macrophages, eosinophils, plasma cells, neutrophils and mast cells . While studies on myocardial biopsy fragments from chronic Chagasic patients indicate a predominance of CD8+ over CD4+ T cells T. cruzi infection also causes a decrease in expression of lymphocyte surface molecules including CD3, CD8, and CD4 in order to circumvent host immunity. Questions remain pertaining to the cytokine environment produced during chronic infection. While some argue that heart-infiltrating T cells yield only a significant production of IFN-ó and TNF-ñ, contributing to IL-12 synthesis and control of the infection, others claim that macrophage IL-10 production facilitates the replication and survival of the pathogen. Interestingly, parasites are rarely found in the hearts of chronic Chagasic patients, yet parasite DNA can be detected in some inflammatory lesions. Through an uncertain mechanism, myocyte destruction continues throughout the course of disease, causing the gradual accumulation of fibrosis and decreased contractility of the heart. The diminished muscle mass, rhythm irregularity (arrhythmia or ventricular tachycardia), and ultimate heart failure is the leading cause of death in chronic Chagas patients. In fact, 10% of all T. cruzi infected patients will die from refractory, end-stage heart failure or severe arrhythmia (26, 27), giving chronic Chagas disease patients a shorter survival and worse prognosis than cardiomyopathies of non-inflammatory etiology. Current chemotherapeutic approaches for the specific treatment of Chagas disease are considered to be unsatisfactory because of frequent toxic side effects and overall limited efficacy, particularly in the chronic form of the disease(Revelli, 1999). In fact, the irreversible nature of the diminished cardiac contractility observed in the chronic phase of Chagas makes heart transplantation the only viable therapeutic option. The frequent side effects of currently accepted treatments, benznidazole and nifurtimox, likely result from bystander reductive or oxidative damage in mammalian tissues that is intended to specifically exploit the deficiency of detoxification mechanisms in T. cruzi. While the use of these nitroderivatives has had limited success in the treatment of acute infection, physicians have been hesitant to prescribe such treatment since complete eradication of T. cruzi is uncommon using such measures. When employed for the treatment of chronic Chagas disease, these therapies were unable to prevent lesions of the heart and digestive tract and had no impact on mortality after 10 years of administration. Unfortunately, rather than prescribing what is clearly an insufficient treatment for chronic Chagas, physicians are forced to treat symptoms as they appear instead of the disease itself.
ReferencesRevelli, S., C. Le Page, E. Piaggio, J. Wietzerbin, and O. Bottasso. 1999. Benznidazole, a drug employed in the treatment of Chagas' disease, down-regulates the synthesis of nitrite and cytokines by murine stimulated macrophages. Clin Exp Immunol 118:271-277.
Murta, S. M., C. Ropert, R. O. Alves, R. T. Gazzinelli, and A. J. Romanha. 1999. In-vivo treatment with benznidazole enhances phagocytosis, parasite destruction and cytokine release by macrophages during infection with a drug-susceptible but not with a derived drug-resistant Trypansoma cruzi population. Parasite Immunol 21:535-544.
Prata, A. 1994. Chagas' Disease. Infect Dis Clin North Am 8:61-77.
Moncayo, A. 1999. Progress towards interruption of transmission of Chagas disease. Mem Inst Oswaldo Cruz 94 Suppl 1:401-404.
 Sencer points to a depiction of Triatomine sp., wh...
Sencer points to a depiction of Triatomine sp., wh... Trypanosoma forms in blood smear from patient with...
Trypanosoma forms in blood smear from patient with... Carlos Chagas, em seu laboratório no Instituto Os...
Carlos Chagas, em seu laboratório no Instituto Os...