Travelers Beware! Do not drink the local water or milk. Cook all foods that may
have been exposed to water. Do not eat uncooked salads, fresh fruit, or shellfish. Why are
so many travelers to third world countries getting these warnings? The answer is simple,
due to the infectious bacterial disease known as Cholera.
Cholera is caused when the bacterium Vibrio cholerae infects the small intestine. A
more precise name for the region infected is the gastrointestinal area. The bacterium itself
is small, and comma-shaped (see appendix p.7 ). Vibrio cholerae is a gram-negative
bacteria that is a pathogen of humans. The bacteria moves by means of flagellum. The
bacterium produces a toxin that causes the small intestine to secrete fluids, leading to
vomiting and diarrhea. The life cycle of the cholera bacterium is simple; Vibrio cholera
reproduces by binary fission, a form of asexual reproduction. The genus, Vibrio, are
typically marine organisms that are found on the surface of the water.
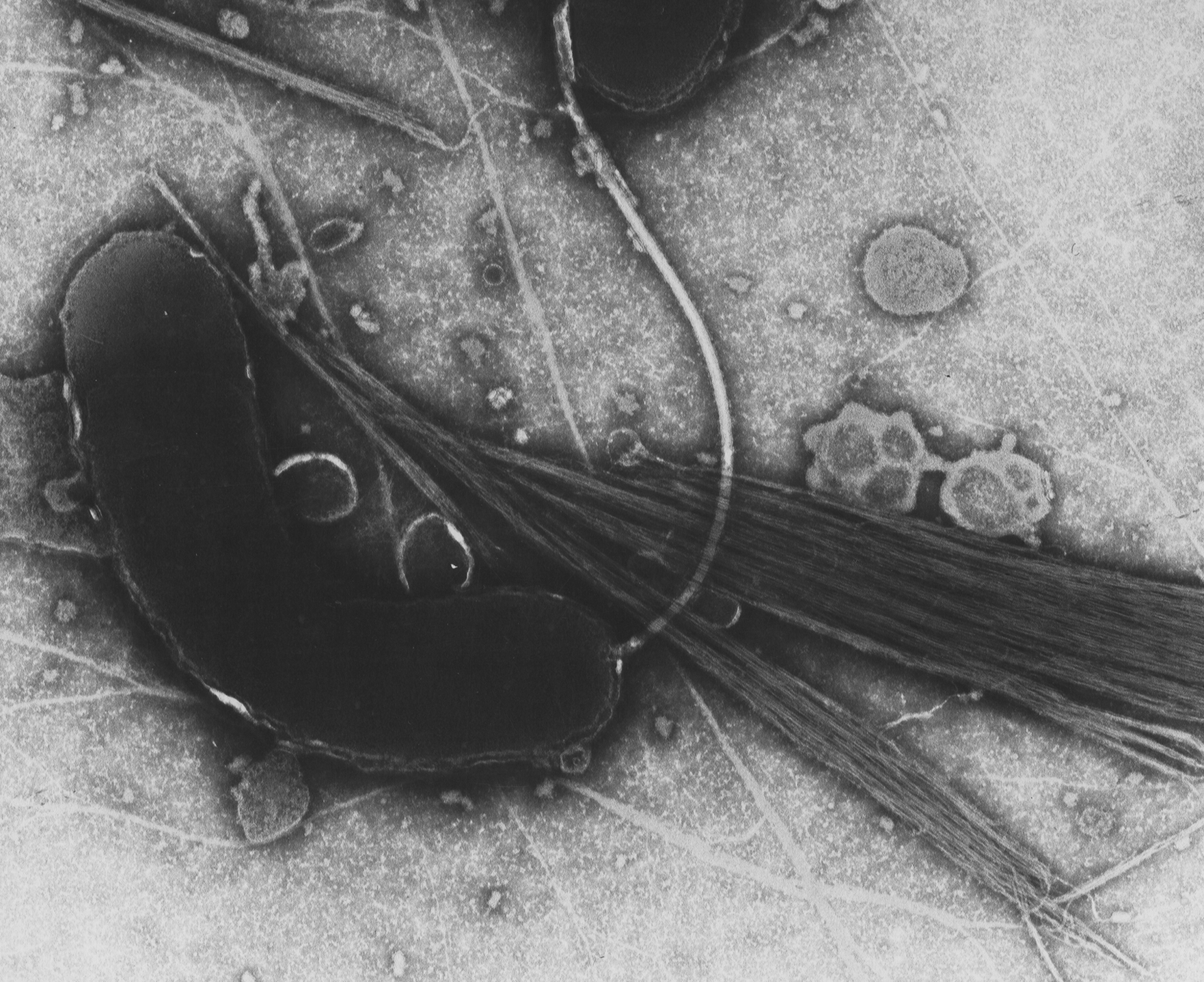 Vibrio cholerae, the bacterium that causes cholera...
Vibrio cholerae, the bacterium that causes cholera... cholera prevention sign board
cholera prevention sign board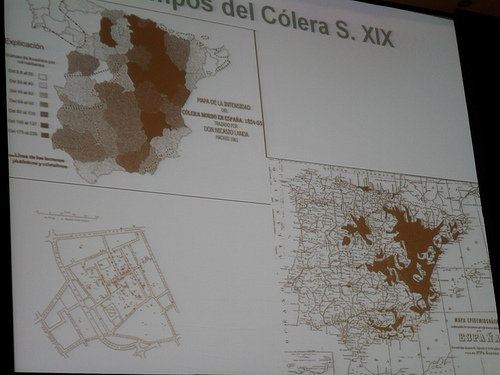 Cholera outbreaks in Spain
Cholera outbreaks in SpainThe cholera bacteria
is usually found in the same water as feces. The bacteria, once ingested by humans, begins
to produce a Cholera toxin. Cholera toxin activates specific enzymes in intestinal cells,
which leads to the secretion of fluids into the small intestine, causing symptoms like
diarrhea. Most of the bacterium are not able to survive the secretions and low pH of the
stomach; after the release of the Cholera toxin, the bacterium usually die.
The first true case of cholera was recorded in Europe in 1830 and again, in 1848,
1854, 1865, 1884, and 1892. During the terrible London epidemic of 1854, John Snow,
proved cholera to be a waterborne disease, through epidemiological means. The first
major U.S. epidemic occurred in the Mississippi Valley from 1870-1873. In 1884, Robert
Koch, a German scientist, discovered Vibrio cholerae as the cause of the disease. An
outbreak in Hamburg, in 1892, was concluded to be caused by pollution of the Elbe River.
For the first half of this century, cholera was confined to Asia, except for an epidemic in
Egypt, in 1948. Control of cholera is still a major problem in several Asian counties.
Epidemics occurred in Calcutta, India in 1953; between 1964 and 1967 in South Vietnam;
and for the Indian refugees of the civil war of 1971, of which 6,500 people were killed. In
the early 1990's, an epidemic occurred in seven South American countries. There were
342,000 documented cases of the disease and 3,600 deaths. Cholera is rare in the United
States. The few cases that do arise each year involve travelers returning from Asia or
Africa, or from imported goods from the Gulf of Mexico area. Cholera occurs naturally in
the Gulf of Mexico, and each year several cases in the U.S. result from shellfish caught in
those waters. The first cholera vaccine was invented in 1981 in the United States. The
O139 variant of the cholera bacterium was discovered in 1992. This produces a more
active form of the disease. The people of India that have become immune to the earlier
strain of cholera have been infected by the O139 bacterium. In 1994, 10,000 refugees of
the Rwandan civil war died from cholera. Even though major outbreaks may not be likely
in the United States, in other countries a small outbreak may flare up to be a major
epidemic.
The symptoms for cholera usually first appear one to three days after initial contact
with the bacteria, usually through means of ingesting it. The first symptoms a carrier of the
disease might have are mild dehydration, nausea, dizziness, and anxiousness. The next set
of visible symptoms are watery diarrhea, and vomiting, which ranges in levels of
seriousness. As much as a pint of water an hour can be lost as the diarrhea continues. In
more serious and severe cases of cholera, symptoms include very intense vomiting, intense
thirst, painful cramps, and cold and withered skin. No matter how serious a case of
cholera is, there is usually no fever. Whenever the first symptoms start to appear, the
person should contact a physician immediately. If a physician suspects that you have
cholera, he will need a sample of your watery stool, which he will then send off to a
medical lab, in order to confirm if you have contacted the disease.
Treatment for cholera is almost one hundred percent successful. The key step in
the treatment is full replenishment of all the lost fluids. This rehydration must be prompt,
as not to cause further sickness or injury to the patient. Patients can be treated with an oral
rehydration solution, a pre-packaged mixture of sugar and salt that is mixed with water
and ingested in large amounts. This solution is used all over the world to treat diarrhea.
Severe cases of the disease require intravenous replacement of liquids. Fluid therapy must
be continued until all lost liquids are replaced and the diarrhea stops. Some medicines can
be purchased, such as Tetracycline, that shorten the duration of the diarrhea. With prompt
treatment, fewer than one percent of cholera patients die. Without treatment, death can
come as soon as forty-eight hours after initial infection, and in big epidemics, the death
rate has been known to exceed sixty percent.
A cholera vaccine is available; however, it is not normally recommended. Only fifty
percent of those that take the vaccine develop immunity to the disease, and for those who
do develop immunity, it only lasts a few (about two to six) months. Complete vaccination
against the disease requires two doses of vaccine taken one to four or more weeks apart.
Cholera doses are age specific. The cholera vaccine is not recommended for infants or
pregnant women. Reactions to the vaccine are: erythema, fever, malaise, and headaches.
Serious reactions are rare, but if experienced, it is strongly recommended not to
revaccinate. No country currently requires the cholera vaccine for entry and departure to
and from cholera-infected areas.
Prevention of cholera is very easy; just be educated and aware. In places where
there is adequate water purification and filtration, and where there is good food sanitation,
cholera is rare. However, in places that lack these qualities, travelers need to take
precautions. People should avoid drinking water from untreated areas (i.e. streams, lakes,
rivers, and ponds) or water from unknown sources. People should wash their hands
thoroughly with soap and cleanser after using the bathroom, changing diapers, and before
preparing foods. Travelers should remember to cook all foods, and to eat them promptly
after their preparation. Also, when available, drink bottled water over non-bottled.
Travelers should stay away from the local foods. Ice in drinks can be harmful as well.
Over the long term the surest prevention of cholera will come with improved sanitation.
Because cholera has a near one hundred percent recovery rate when treated
promptly, and treatment for the disease is easy, it is no wonder that there has not been a
major effect on world population or health from this disease. The most deadly epidemic of
cholera occurred in a worldwide chain of epidemics in the early 1800's, killing an
estimated three million people. This is very small considering the millions of people
that die from AIDS today. The second most deadly epidemic was in 1971, when
Bangladeshi refugees fled from India during their civil war. 6,500 people were killed. The
third most deadly epidemic was in 1991. Outbreaks of cholera in Peru quickly spread to
other South and Central American countries, including Mexico. In this epidemic 340,000
cases were reported, and 3,600 deaths were confirmed. Despite the large epidemics, the
world's population and health has not been greatly effected by cholera.
The immune system responds to the disease causing organism with a whole
spectrum of responses. The reasons for this big spectrum is not known. One response is
after infection, antibodies can be detected against cholera antigens including the Cholera
toxin that Vibrio cholerae makes. Antibodies detected against cholera antigens are
considered "Vibriocidal" antibodies because they will lyse V. cholerae cells along with
complement and serum components. Vibriocidal antibodies reach a peak 8-10 days after
initial infection, then decrease, returning to the baseline 2-7 months later. The presence of
V. antibodies goes along with a resistance to infection; however, the antibodies may not
be the relayer of this protection, and the role of circulating antibodies in natural infection is
unclear.
The cholera bacterium evades the immune system simply by traveling too fast for
it. The bacteria is ingested, goes to the small intestine were it releases its toxin, and then is
killed by the stomach's low pH secretions, prior to the immune system having a chance to
respond.
There has not been an active case of cholera in the United States for nearly 90
years. The U. S. has had fewer than 80 proven cases of cholera ever, most of which
were brought into the country by travelers returning from South America. No major
outbreaks of this disease have occurred in the U.S. since 1911. However, small cases
occurred in 1973 and 1991, due to poorly prepared shellfish that were imported to the
United States from the Gulf of Mexico area. The excellent sanitation facilities in the U.S.
translate into the near elimination of the chance of an epidemic of cholera ever occurring.