Medical History of Tuberculosis
Tuberculosis is a disease that holds a significant amount of history within the United States, as well as the rest of the world. It is a disease that has ravaged and afflicted society throughout recorded history and can be traced back to the Stone Age.
History of Tuberculosis : Throughout history, tuberculosis has been given a variety of names; however, there is one unifying strand evident in the uniform documentation of symptoms. Recently, fragments from the spinal column of Egyptian mummies have been found to show clear pathological signs of tubercular decay. The disease was first referred to as Pthisis by the Greeks in 460 BC, meaning literally "to waste away." Hippocrates, noted philosopher and physician who was known as the "Father of Medicine," identified it as the most widespread disease of the time and pointed out its high fatality rate. Due to the high case-fatality rate, he warned physicians to refrain from visiting patients in the late stages of disease progression, due to fear of damaging the physician's reputation.
 English: Photomicrograph of a sputum sample contai...
English: Photomicrograph of a sputum sample contai...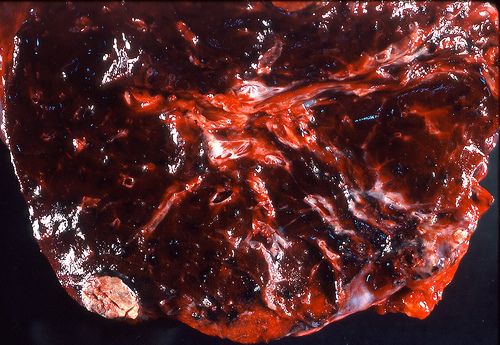 Tuberculosis - Sub-pleural primary (Ghon) focus
Tuberculosis - Sub-pleural primary (Ghon) focus Tuberculosis Hospital (demolished)
Tuberculosis Hospital (demolished)During the 17th century, pathological and anatomical descriptions of tuberculosis began to emerge. In 1679, Franciscus Sylvius was the first individual to identify actual tubercles as a consistent and characteristic pathological change in the structure of the lungs. He also went on to describe their progression to abscesses and cavities. Following the publication of his discovery, descriptions of the infectious nature of this disease began to emerge in Italian medical literature.
In 1720, Benjamin Marten, a prominent English physician, became the first to propose a completely new theory for the etiology of this disease. In his work, A New Theory of Consumption, he talks about his belief regarding transmission of TB. He writes:
It may be therefore very likely that by an habitual lying in the same bed with a consumptive patient, constantly eating and drinking with him, or by very frequently conversing so nearly as to draw in part of the breath he emits from the Lungs, a consumption may be caught by a sound person...I imagine that slightly conversing with consumptive patients is seldom or never sufficient to catch the disease.
Medical researchers point out that Marten demonstrated a significant amount of epidemiological insight for that time period. Although strides were slowly being made in understanding the etiology of this disease, researchers, desperately searching for a cure, continued to search unsuccessfully and hope for a breakthrough.
In 1839, this mysterious disease was finally given the name of tuberculosis by a man named Johann Schonlein. The year, 1854, brought significant progress in the struggle to understand this devastating disease. A Silesian botany student by the name of Herman Brehmer was instructed by his attending physician to seek out a healthier climate after struggling with TB. He followed this advice by traveling to the mountains of Himalaya where he continued to study botany with the hope of finding better health. After spending time there, he returned home healthy and with a strong desire to study medicine. In 1854, his presented his doctoral dissertation entitled, "Tuberculosis is a Curable Disease." That same year, he built an institution in an environment similar to the one he had experienced that provided patients suffering from TB with an environment that aided them in their battle against this disease. Tucked far away from the city and the problems that urbanization had created, this institution offered nature, fresh air, good nutrition, and wide-open spaces as a remedy for TB. Brehmer's creation quickly became a model for the development of similar institutions and was integral in laying the foundation for the sanitarium movement that was soon to follow.
Not long after this significant development in the fight against TB, new advances quickly followed. In 1865, Jean-Antoine Villemin, a French military doctor, demonstrated that the disease was transmitted from humans to cattle and from cattle to rabbits. This evidence became revolutionary, and he went on to postulate that a specific microorganism was the cause of the disease, which put an end to the previous theories regarding the spread of the disease.
In 1882, Mycobacterium Tuberculosis, the infectious agent that causes TB, was discovered by a German microbiologist named Robert Koch. Following this breakthrough, the previous romanticized idea of this disease began to significantly decline, bringing with it a widespread hope that a cure for this disease would soon be found.
During the 1890's, the second leading cause of death was tuberculosis, barely falling beneath the leading causeâÂÂpneumonia. At the beginning of the 19th century, another key development in the fight against TB came about through the work of two French scientists-Calmette and Guerin. After long hours and careful research, they succeeded in developing a vaccine consisting of living tuberculosis germs. In 1921, the vaccine was officially named BCG after the two scientists who had produced it.
During World War II, a noteworthy breakthrough in the fight against this disease finally occurred with the development of chemotherapy. The current use of chemotherapy to combat infectious disease had not been effective against tuberculosis until a scientist named Selman A. Waksman at the University of California began routinely screening soil bacteria and fungi and noticed the effect that fungi had on bacterial growth. In the year 1940, he isolated an effective anti-TB antibiotic named actinomycin. Unfortunately, however, this proved too toxic for use in either animals or humans. In 1943, his perseverance paid off, and animal tests of streptomycin revealed low toxicity. On November 20, 1944, the antibiotic was administered for the first time to a patient who was seriously ill. The effects were almost immediate. The disease was halted from progressing any further, bacteria disappeared from the sputum, and the patient made a rapid and complete recovery. Over the next few years, a steady flow of new anti-TB drugs appeared. This was important because resistant strains were already developing with the use of streptomycin which endangered the success of future antibiotic therapy. However, it would later be demonstrated that the danger of mutant strains could be overcome by the combination of more than one anti-TB drug.
Another turning point in the struggle to combat/treat TB was the development of the chest-x ray in 1895. This allowed physicians to study the condition of the lungs and follow the course of the disease.
Pathology of the disease: TB is primarily an illness of the respiratory system and is spread by coughing and sneezing. Transmission occurs with infectious TB vs. latent TB. When a person infected with TB coughs/sneezes, he/she exhales bacilli into the air, and another person need only inhale a small number to get infected. If an individual with active TB is left untreated, he/she is likely to infect between 10-15 people with the disease. Those who become infected may not become sick right away. The disease often lies dormant for years and then chooses to emerge at a later stage in life.
TB as a global epidemic: Although progress has been made in the fight to control this disease, within the last few years, TB has quickly turned into an epidemic of global proportion. The number of new cases, globally, correlates with poor economic conditionsâÂÂthe majority being documented in developing countries. The World Health Organization estimates that over 800,000 people get TB every year, and over 95 percent of those individuals live in developing countries. Overall, TB account for between 2-3 million deaths worldwide.
HIV/TB : HIV has been shown to significantly alter the epidemiology of TB, and the combination of the two has proven to be lethal, particularly in the developing world. TB is now a leading cause of death for individuals who are HIV-positive. In Africa, HIV has been the single most important factor in evaluating the increased incidence of TB over the past ten years.
Multi-drug resistant TB: Recently, we have seen the resurgence of TB due to the development of multi-drug resistance. Drug resistance develops due to incomplete/partial treatment when patients do not complete their prescribed drug regimen. This may be due to a variety of factors such as patients feeling they are no longer sick and therefore do not need to finish the medication, lack of availability, or the physician may have prescribed the wrong drug. Public health specialists are careful to point out that poorly supervised or incomplete treatment of TB is often worse than no treatment at all, due to the consequences of MDR. Drug resistance is particularly difficult to control in the developing world, due to the lack of appropriate systems being in place. In order to fight this new battle, the WHO proposes that the recommended way to cure TB is by means of Directly Observed Therapy (DOTS). The DOT system is an inexpensive prevention program that follows careful supervision of a patient's treatment, including direct observation of drug intake, as one of its main objectives. This approach has shown to be highly effective since its implementation, with the World Bank identifying it as one of the most "cost-effective of all health interventions."
Many scientists speculate that tuberculosis is a disease that has been present in society since the beginning of time. Today, tuberculosis continues to pose a serious health threat, and it is vital that the world come together in solidarity so we can continue to see success in our efforts to control virulence and transmission.
Bibliography
Top of Form
CDC. <http://www.cdc.gov/nchstp/tb/faqs/qa.htm>.
Drug- and Multi-resistant Tuberculosis (MDR-TB). World Health Organization. <http://www.who.int/tb/dots/dotsplus/en/>.
Entin, MA. Romance and tragedy of tuberculosis: Edward Archibald's contribution to the surgical treatment of pulmonary tuberculosis. Winter 1995, Volume 3, Number 4. <http://www.pulsus.com/Plastics/03_04/enti_ed.htm>.
Gupta R, Espinal MA, Raviglione MC. Tuberculosis as a major global health problem in the 21st century: a WHO perspective. Semin Respir Crit Care Med. 2004 Jun;25(3):245-53. PMID: 16088467 [PubMed].
Maher D, Raviglione M. Global epidemiology of tuberculosis. Clin Chest Med. 2005 Jun;26(2):167-82, v. Review. PMID: 15837103 [PubMed - indexed for MEDLINE].
Nunn P, Williams B, Floyd K, Dye C, Elzinga G, Raviglione M.Tuberculosis control in the era of HIV. Nat Rev Immunol. 2005 Oct;5(10):819-26. Review. PMID: 16200083 [PubMed - indexed for MEDLINE]<http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=PureSearch&db=PubMed&details_term=%28%28%22tuberculosis%22%5BMeSH%20Terms%5D%20OR%20tuberculosis%5BText%20Word%5D%29%20AND%20raviglione%20m%5BAuthor%5D%29>.
Tuberculosis. World Health Organization. <http://www.who.int/mediacentre/ factsheets/fs104/en/index.html>.
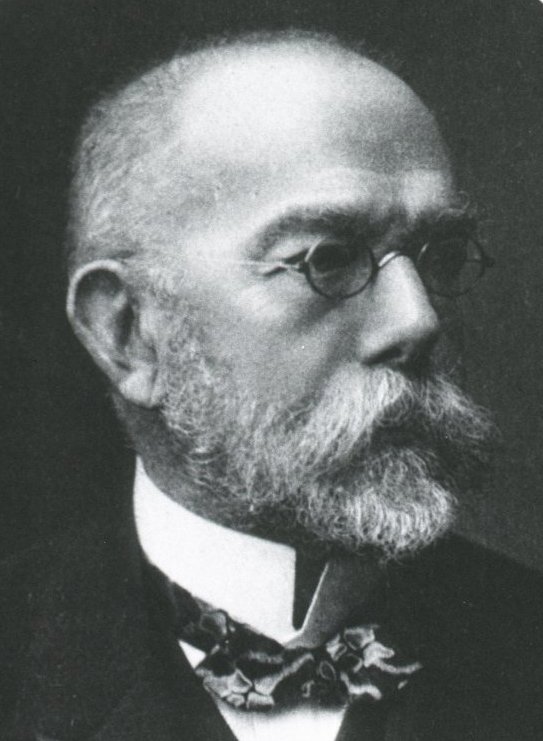 Portrait of Robert Koch (1843—1910).
Portrait of Robert Koch (1843—1910). None - This image is in the public domain and thus...
None - This image is in the public domain and thus... The Mantoux skin test consists of an intradermal i...
The Mantoux skin test consists of an intradermal i... Dr. Selman Waksman, half-length portrait, facing l...
Dr. Selman Waksman, half-length portrait, facing l...