Modern wound management is a challenging and rewarding area of clinical practice for the student nurse. This modern approach involves simple advances in practice. Firstly, modern wound management uses moist wound healing processes that have been researched and determined to be significantly more effective than the dry healing of the past. Secondly, and more importantly, it is a more holistic approach that looks at more than the wound itself, but addresses the whole patient in medical, environmental and social contexts Waldrop, Doughty, (2000).
Most sources indicate that wound healing is made up of an orderly sequence of events. This, in turn, is characterised by specific movement of specialised cells into the wound, carrying out specific tasks Bale, Harding, Leaper, (2000). According to the movement of the cells and the orderly sequence of events in healing is regulated by cytokines or growth factors.
The healing stage of photo 3 appears to be the Proliferative (or regeneration) stage.
 English: Phases of wound healing. Limits vary with...
English: Phases of wound healing. Limits vary with... wound healing in Drosophila. Cropped
wound healing in Drosophila. Cropped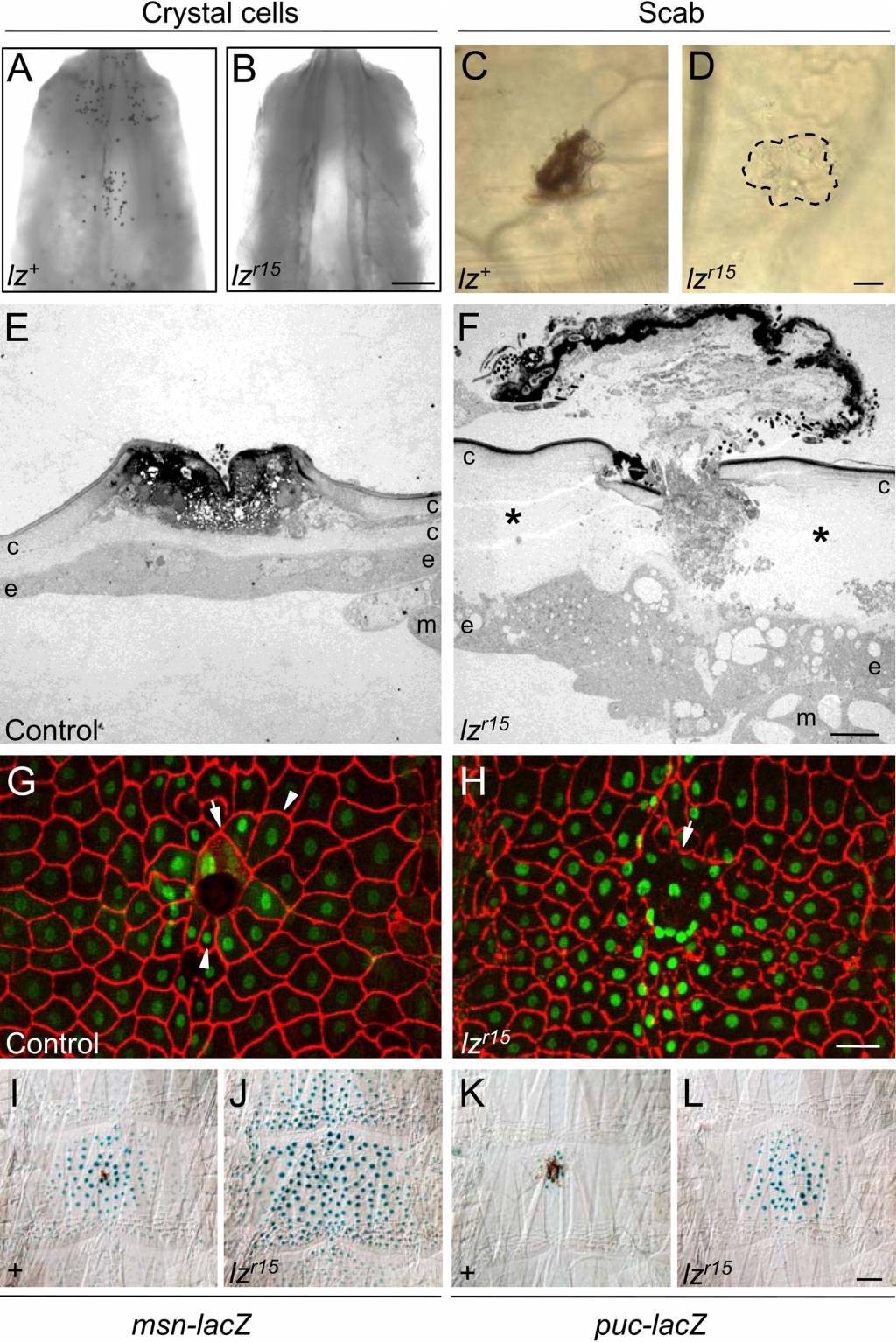 wound healing in Drosophila
wound healing in DrosophilaEvidenced by its colour - bright red, moist and shiny appearance. As a student nurse it would always be well off to remember that healing is a continuum of complex connected processes that are divided into phases. These phases are known as the inflammatory phase, the proliferative phase, the maturation phase.
This essay will list the series the events that occur during the granulation, epithelisation and contraction stages of the proliferative phase.
Granulation
Also known as Angiogenesis, which is the growth of new blood vessels
(Bale et al. 2000). Is an essential ingredient for regeneration of granulation tissue. Tissue hypoxia (low oxygen) sets in following disruption to the blood flow on injury, stimulating macrophages to secrete a substance known as angiogenesis factor. The process of angiogenesis is delayed if a thick layer of surface necrosis is present
Waldrop et al. (2000).
According to Hopkinson (1992) undamaged capillaries beneath the wound produce buds, stimulated by growth factors, these buds form a network of loops, which fuse with other buds to form a new capillary bed. These new loops are fragile and can be easily damaged Dealey (1994). Some types of dressing made of open weave cotton such as gauze become stuck to the granulating tissue and on removal could damage the new capillary loops. I will discuss more about gauze in the following paragraphs.
If the wound edges are close, the capillaries can bridge the wound. This new tissue is known as granulating tissue. However this process can be impaired by excess inflammation, dead surface tissue, wound exudates, decreased perfusion, and corticosteroids-A steroid hormone produced by the adrenal Dealey (1994).
Epithelialisation
This describes the phase where the wound is covered epithelial tissue. At the edges of wounds, epidermis begins to thicken. The migration marginal basal cells across the wound bed begins, along fibrin strands stopping when they come in contact with each other (contact inhibition) Waldrop et al (2000).
This movement only occurs on a moist surface, under a scab or a dressing that provides a moist environment Winter (1999). Therefore the wound surface should be kept hydrated. The depths of the wound at this point contain inflammatory cells and fibrin strands, as the epithelial surface thickens these are joined by a new cell type, the fibroblast. Which is released from macrophages and platelets Winter (1999). Fibroblast synthesis's and secretes collagen (a fibrous protein).
Endothelial cells nearest to the injury spread out into the wound and bring rapid capillary proliferation Winter (1999). These cells then activate fibrinolysis, ending the earlier produced fibrin network, clearing the way for fibroblast migration and their collagen production, Waldrop et al (2000).
Contraction
Next in sequence is wound contraction, the process whereby open wounds close by movement of the wound edges (not just epithelium) toward the centre, in an attempt to reduce the surface area of the wound. Hunt and Dunphy (1969) described wound contraction as a "remarkable physiological event that leads to spontaneous closure of open lesions". Unlike granulation tissue formation the process of wound contraction is less depending on the general condition of the organism Bale et al (2000).
Wound contraction is mediated by fibroblasts of the granulation tissue. Under certain conditions fibroblasts can convert into a cell type that shares many structural and functional features with smooth muscle cells, including the formation of the contractile smooth muscles protein actomyosin Bale et al (2000).
Carville (1994) explains that the main objective in applying a dressing is to create an environment that is conductive to healing. Therefore as a student nurse it is important to understand the physiology of wound healing, the ideal dressing should be chosen.
Natural fibre dry dressing, such as gauze are used as primary or secondary dressing for absorbency or wound protection. They can be used for compress or continuous wet dressing. However, according to Carville (1994) gauze is not considered to be an
'ideal dressing' as it provides a "dry" warm environment. Winter (1999) demonstrated that epithelisation of a wound occurs more rapidly if a most wound environment was maintained. Gauze dressing was found to shed fibres into the wound which provides focus for infection. Fragile tissue cells can easily be damaged following the removal of this type of dressing, further more exudate may strike through the dressing allowing pathogen to enter the wound further complicating the healing process.
Waldrop et al (2000) listed the following reasons for applying a dressing are "to create an environment that promotes healing, this is best done if the wound site is kept moist by using appropriate dressing. Reducing pain by excluding air from exposed nerve endings, benefiting the comfort of the patient".
When wounds do not heal, there is an increase in discomfort that impact with the quality of life in patients. According to Waldrop et al (2000) this often leads to long-term disability and an increase in the risk for additional medical problems. Before the underlying causes of the problem can be addressed the wound must be debrided or cleaned.
Dressings and other treatments should be designed around the patient and consider such things as the ability to wear normal clothes and maintain a reasonable body image. Dealey (1994) stated that, "focusing on the patients needs in respect of the wound should be the aim of treatment". With a careful selection of dressing products to afford good wound control and with good care of the skin the impact of a non-healing wound on the patients lifestyle can be minimised.
To conclude, open wounds have many different tissue appearances, and the treatment objectives for each phase may require a different approach. In addition, the wound may produce differing amounts of problems in its various phases, which must be managed in an appropriate fashion. This influences the type of dressing that is selected for the treatment of the patient's wound. Non-healing wounds may be due to physiological problems or other factors which needs to be identified and addressed where possible, to improve healing ability and overall quality of life for the patient.
References
Bale, S., Harding, K., Leaper, D. (2000) An introduction to Wounds. London: Emap Healthcare.
Carville, K. (1994) Wound management - an art and a science. New England: University of New England Press.
Cherry, G., Harding, K., Ryan, T. (2000) (eds). Wound Bed Preparation
(International Congress and Symposium Series 250). London: Royal Society of Medicine Press.
Dealey, C. (1994). The Care of Wounds. Oxford: Blackwell Scientific Publications.
Hopkinson, I. (1992) Growth factors and extracellular matrix biosynthesis. Journal of Wound Care 1:2, 47-50.
Harding, K. (1998) (eds) Wounds: Biology and management. Oxford: Oxford Medical Publications.
Waldrop, J., Doughty, D. (2000) Wound healing physiology. In: Bryant R (ed). Acute and Chronic Wounds: Nursing management (2nd ed). Missouri: Mosby.